





My slim, 88-year-old female patient said, "My doctors have told me that I should keep up whatever I am doing." Joan had stopped taking Boniva, the drug prescribed for her osteoporosis when she came to our clinic more than two years earlier.
By January 2008, approximately 3 months after beginning bioelectromagnetic and laser treatment, Joan's bone density had increased by 0.5 percent at L1-L4, the area of severe osteoporosis. By December 2009, she had gained another 8.8 percent bone density in her lumbar spine, It is important to understand that individuals with severe osteoporosis typically experience frequent, intermittent back pain due to "compression" fractures that can occur spontaneously in weakened bone. Joan seldom has pain these days and has reported better overall health, energy and ability to exercise.
Osteoporosis is "systemic skeletal disease characterized by low bone mass and micro architectural deterioration of bone tissue, with consequent increase in bone fragility and susceptibility to fracture risk." According to estimates by the National Osteoporosis Foundation, 10 million Americans (8 million women and 2 million men) have osteoporosis, and almost 34 million more (55 percent of those over age 50) are at risk of developing it. In 2005, osteoporosis-related fractures cost $19 billion, and costs are predicted to rise to approximately $25.3 billion by 2025.
Twenty years ago osteoporosis was usually diagnosed only after a fracture. Nowadays, bone mineral density (BMD) can be measured by a type of x-ray technology called dexascan. To qualify as osteoporosis, bone density must be < -2.5 standard deviations than that which is normal in a young adult of the same sex. The number itself is called a "T-score."
Joan's T-scores of -3.3 (serious bone loss) in October 2006 and January 2008 were far below the -2.5 level defining osteoporosis. In contrast, her T-score of -2.7 in December 2009 shows stunning improvement and is very close to the -2.5 borderline. Based upon her progress, it is easy to believe that her bone density will be normal, or nearly so, on her next dexascan in two years.
Osteopenia is milder bone loss, described as, "Low bone mass. Defined as -1.00 to -2.49 standard deviations below the average peak adult bone mass as determined by a bone mineral density examination." Few people had ever heard the word osteopenia, much less received treatment for it prior to 1995. Yet today millions of women worldwide are taking biphosphonate drugs because they believe their condition requires it. To learn how osteopenia became a popular medical diagnosis, visit "How A Bone Disease Grew To Fit The Prescription."
Normal Bone Formation Vs. Biphosphonate Effects
In normal bone formation, as a matrix of new connective tissue is laid down by osteoblasts and then mineralized, old bone is removed by osteoclasts. Like in any living tissue, older cells are continually replaced by newer ones. Biphosphonates disrupt this. They suppress the resorption of old bone, inhibiting and even killing osteoclasts. Without the normal actions of osteoclasts to remove old bone, the bony tissue resulting from long-term biphosphonate use, though denser on x-ray, is often weaker, less vascular and more prone to serious adverse events such as spontaneous stress fractures, esophageal cancer and biphosphonate-related osteonecrosis of the jaw (BRONJ).
In BRONJ the maxillo-facial bones become necrotic. It is ironic and sad that so much destruction is wreaked upon bones by drugs intended to strengthen them. It is doubly ironic that laser therapy has been shown to effectively treat the consequences of BRONJ: "Of the 14 patients who underwent laser biostimulation, nine reported complete clinical success (no pain, symptoms of infection, or exposed bone or draining fistulas), and three improved their symptomatology only, with a follow-up of between 4 and 7 mo. CONCLUSIONS: While the results reported in this study are not conclusive, they indicate that laser therapy has potential to improve management of BON (Biphosphonate-related osteonecrosis of the jaw)."1
Building Bone Safely and Cost-Effectively
Laser and bioelectromagnetic therapies are osteogenic; they stimulate osteoblasts to form new bone.2-6 The resulting tissue may be stronger and more flexible than the original. In contrast, biphosphonates inhibit normal breakdown of old bone. When given a choice of new or old bone, which would you choose to have more of for yourself or your patients?
 Laser therapy may be administered by probe treatment, laser needle acupuncture and other methods. It may provide rapid pain relief and accelerate bone healing in specific areas, even with severe bone loss. Whereas laser therapy is labor intensive, bioelectromagnetic therapy may be given over large areas, even the whole body, as an unattended treatment. It may also be the most cost-effective means for home treatment. Both laser and bioelectromagnetic therapies are wonderful clinical tools, which, in combined treatment, may complement and enhance one another.
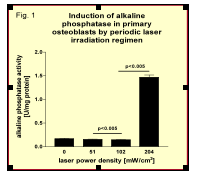
When laser light is given at relatively low average output powers but concentrated to achieve high intensities, it may significantly stimulate osteoblasts. The induction of alkaline phosphatase by osteoblasts is associated with bone formation. Haxsen, et al., compared the effects of dose and intensity of laser needles to stimulate alkaline phosphatase activity and found that once threshold was achieved, the response was logarithmic and that intensity had greater relevance than dose.7
Laser therapy may be administered by probe treatment, laser needle acupuncture and other methods. It may provide rapid pain relief and accelerate bone healing in specific areas, even with severe bone loss. Whereas laser therapy is labor intensive, bioelectromagnetic therapy may be given over large areas, even the whole body, as an unattended treatment. It may also be the most cost-effective means for home treatment. Both laser and bioelectromagnetic therapies are wonderful clinical tools, which, in combined treatment, may complement and enhance one another.
When laser light is given at relatively low average output powers but concentrated to achieve high intensities, it may significantly stimulate osteoblasts. The induction of alkaline phosphatase by osteoblasts is associated with bone formation. Haxsen, et al., compared the effects of dose and intensity of laser needles to stimulate alkaline phosphatase activity and found that once threshold was achieved, the response was logarithmic and that intensity had greater relevance than dose.7
In the study, primary osteoblasts showed no induction of alkaline phosphatase activity using single laser needle stimulation with a laser power density of 51 mW/cm2, an increase of about 43 percent at 102 mW/cm2 power density (two needles per well) and a nine-fold increase at 204mW/cm2 laser power density (four-needle stimulation per well).7
Anyone treated for bone loss should have a vitamin D level assessed by the 25(OH)D test at the outset. Supplementation with higher dosages of D3 based on the results of this test is rapidly becoming the standard of care and may help your patients gain bone mass quickly. If possible, assess bone mineral density before and after a treatment series. Six months is the minimum time to expect significant change in bone density. With good information, the right choices become easy. Teach your patients about the effects of laser and bioelectromagnetic therapies, and also about the negative effects of biphosphonates. Given the choice of new or old bone, which treatment do you think they will choose?
References
- Vescovi P, Merigo E, Manfredi M, et al. Nd:YAG laser biostimulation in the treatment of bisphosphonate-associated osteonecrosis of the jaw: clinical experience in 28 cases. Photomed Laser Surg 2008 Feb;26(1):37-46.
- Kreisner PE, Blaya D, Gaião L, et al. Histological evaluation of the effect of low-level laser on distraction osteogenesis in rabbit mandibles. Med Oral Patol Oral Cir Bucal 2010 Jul 1;15(4):e616-8.
- Saracino S, Mozzati M, Martinasso G, et al. Superpulsed laser irradiation increases osteoblast activity via modulation of bone morphogenetic factors. Lasers Surg Med 2009 Apr;41(4):298-304.
- Márquez Martínez ME, Pinheiro AL, Ramalho LM. Effect of IR laser photobiomodulation on the repair of bone defects grafted with organic bovine bone. Lasers Med Sci 2008 Jul;23(3):313-7.
- Gerbi ME, Pinheiro AL, Marzola C, et al. Assessment of bone repair associated with the use of organic bovine bone and membrane irradiated at 830 nm. Photomed Laser Surg 2005 Aug;23(4):382-8.
- Abo Elsaad NS, Soory M, Gadalla LM, et al. Effect of soft laser and bioactive glass on bone regeneration in the treatment of bone defects (an experimental study). Lasers Med Sci 2009 Jun 23.
- Haxsen V, Schikora D, Sommer U, et al. Relevance of laser irradiance threshold in the induction of alkaline phosphatase in human osteoblast cultures. Lasers Med Sci 2008 Oct;23(4):381-4.
Click here for previous articles by David Rindge, DOM, LAc, RN.