




I don't think you can find land more idyllically beautiful than the high mountains and passes of Kashmir in Pakistan. It was during the holy week of Ramadan, on Oct. 8, 2005, at approximately 9 a.m.
The epicenter was near a town called Gori, 60 miles north of the major city of Islamabad, and not all that far from the line of control. In a matter of 80 seconds, and in the days that followed, an estimated 87,350 people died; 2.5 million were left homeless; and the number of injured grew (as did the bacteria in their wounds). This earthquake was a "shallow" one, beginning only six miles under the earth's surface, thereby making it more deadly while being felt in three different countries. What was considered one of the most beautiful places in the world now lay in ruins, as whole villages were covered with tons of dirt, and shattered houses, schools and shops lay beside and on top of crushed corpses.
 As an acupuncturist/physician assistant/bodyworker, I wanted to do something for the refugees, to help them rebuild their lives and assist in their medical needs. My Western medical training and experiences working in other natural disasters came in handy, but what excited me most was using acupuncture in the midst of this crisis.
As an acupuncturist/physician assistant/bodyworker, I wanted to do something for the refugees, to help them rebuild their lives and assist in their medical needs. My Western medical training and experiences working in other natural disasters came in handy, but what excited me most was using acupuncture in the midst of this crisis.
Prior to these events I had the fortune of meeting Wendy Henry, LAc, of Community Relief and Rebuilding through Education and Wellness (CRREW) while spending some time training to be a National Acupuncture Detoxification Association (NADA) instructor in New York City. Dr. Mike Smith, one of the co-founders of NADA, knew of my interest in bringing the NADA protocol into the military for its use, not just in addiction rehabilitation, but for the treatment of acute anxiety disorder, PTSD, and helping the civilians affected by combat and natural disasters. Dr. Smith hooked me up with Wendy, who works with the New York City Fire Fighters Counseling Services and others who were interested in this application for acupuncture. Wendy had a wealth of information and experience, which she shared with enthusiasm and an infectious, can-do attitude. When Hurricane Katrina blew into Louisiana, Wendy called and put me in touch with people I could work with in New Orleans. Wendy's contacts, along with those of Laura Cooley, LAc, were instrumental in initiating bodywork and acupuncture for exhausted firefighters, police and military service personnel who worked tirelessly while their own homes were destroyed and their families displaced. Wendy and Laura opened the doors for other acupuncturists to enter and work in New Orleans, which was still closed to most civilians. Their example, expertise and successes were noted by mental health care workers and physicians on site, some of whom later were trained as acupuncture detoxification specialists (ADSes).
While working in New Orleans, I met a fellow volunteer, Todd Shea. Our friendship was instantaneous, and respect grew as we saw each other operate. Todd had a natural ability to think outside the box, acquire supplies and equipment for anyone who asked, and did good work with a smile, no matter how difficult the task. Todd spent 45 days in the New Orleans area; when the earthquake hit Pakistan, he was quick to respond to that emergency. Todd and I kept in touch, and he was instrumental in getting me to Pakistan.
Operation Heartbeat, a nongovernmental organization (NGO) started by two physicians from George Washington University, had a medical team in Pakistan by Oct. 16. They recruited 20 physicians with different kinds of medical experience. Their team was headed by Todd, who was responsible for all the logistics, getting new teams in country, and supplying them and other NGOs such as Pakistani Red Crescent and Doctors Without Borders with medicine when needed. The operation was divided into four phases:
- Acute phase - emergency care of survivors
- Subacute phase - emergency outreach into remote, newly accessible and newly identified areas
- Rehabilitative phase - staffing the main field hospital, satellite health units, and outreach teams with local qualified doctors, medical students and other health care professionals
- Reconstructive phase - construction of a permanent hospital at Garhi Dupatta to serve the greater Jhelum Valley
 I arrived in Islamabad and met up with Todd. As our transport hurtled up the bumpy roads, we discussed the current situation and the needs of the local populace. With a new team, we headed to Garhi Dupatta, located in the Jhelum River valley and with mountains on both sides reaching heights of 7,000 to 8,000 feet. As it stood, upon my arrival, Operation Heartbeat's field hospital was only seeing 150 people a day: a marked reduction from the first two weeks, where 450 to 600 patients a day was the norm. The amount of critical injuries also had dropped dramatically, but what was considered necessary were teams to go into the mountains where people were still in need of medical assistance.
I arrived in Islamabad and met up with Todd. As our transport hurtled up the bumpy roads, we discussed the current situation and the needs of the local populace. With a new team, we headed to Garhi Dupatta, located in the Jhelum River valley and with mountains on both sides reaching heights of 7,000 to 8,000 feet. As it stood, upon my arrival, Operation Heartbeat's field hospital was only seeing 150 people a day: a marked reduction from the first two weeks, where 450 to 600 patients a day was the norm. The amount of critical injuries also had dropped dramatically, but what was considered necessary were teams to go into the mountains where people were still in need of medical assistance.
Upon arriving in Garhi Dupatta I started getting medical packs together. Along with the antibiotics, surgical equipment, IV solutions, antidiarrheals, antifungals and antiparasitics went 3,000 acupuncture needles donated by Helio. (Helio was very generous and supplied the project with much-needed supplies.) I was in charge of the medical teams on nine separate operations into the mountains during my stay, with each trip lasting two to three days. Teams consisted of physicians, medical students, an investment banker (who spoke Urdu), surgical technicians and EMTs, paramedics, midwives and a naturopath.
Sorties going into the mountains began by first conferring with the Pakistani Army, which supplied helicopters, ground transportation, and, more importantly, had real-time intelligence of what was needed and where medical help was needed. The Pakistani Army had troops in forward bases where they were supplied with tents, food and bedding brought in by helicopters to distribute to earthquake victims to prepare them for the soon-to-be-arriving winter.
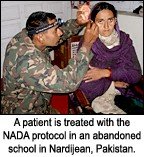
Our first stop was Nardijean, a small village that had lost 289 people in the quake. Five men were still in the landslide easily visible from the village; they were cutting grass for their cows at the time the earth shook. We treated everything from pneumonia and abdominal pain to infected wounds that had not been cleaned or unbandaged for up to three weeks. People who showed overt signs of anxiety or were known to have psychological problems since the earthquake also were asked to come. Our translators did a great job; as people came and were able to get comfortable with us, they began to open up. I spoke to Captain Hammad, who was in charge of the village, and asked his permission to do acupuncture. I also asked the patients. He had no problem with it and showed great interest in the NADA protocol. In fact, as he could see the effect of acupuncture changing people before his eyes, he asked me to teach him how to do it so he could use it on his men. Captain Hammad became the first of four officers and six enlisted men, three medical students from the U.S. and two psychologists that I trained in the NADA procedure. After three days and worsening weather, we had to put on our packs and hike out to the nearest army camp that could get transport for us back to Gahri Dupatta. Our supplies were all but gone, and Todd asked me to get back so we could redeploy to another area.
Once back in base camp, I would get the medical box ready for our next trip. News of the acupuncture got back to base via the grapevine. I was asked by a major to show him the NADA protocol. I asked him to sit on a bunk bed and start a natural breathing cycle. As he did this, I inserted the needles and let him "chill" for 40 minutes. When I pulled out the needles, he looked at me with glazed eyes and asked me to teach him the protocol also. The word was starting to spread among the officers of 212th Brigade that someone was putting needles in people's ears and they were starting to feel more relaxed and some of their body pains were going away. All this came from men who climbed over landslides to get into this valley, who were greeted by total destruction, death and severely injured people. Brigadier General Sherier told me of the suffering he and his men witnessed in the first days as injured people poured out of the mountains into the valleys. The general said it was so painful to see all of the children and women injured, that as he helped the wounded, he would sporadically have to walk away from the scene, cry, and come back to do more work. All of the men I spoke with said the same thing.
While in New Orleans, I had done bodywork on Todd, so he immediately went off and told Brigadier General Amjad of the 10th Brigade that he should come for some bodywork. I took out some essential oils I had brought for such an occasion and worked on the general. He encouraged me to keep doing this kind of work and said that if he could help us in any way, he would. So, we started coming up with Christmas lists of things the camp needed and a list of villages further out that we might try to get to. This is known as the "back-scratching" principle!
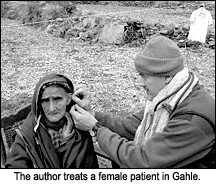
After a month of moving about the mountains of Kashmir, I started reflecting on the work accomplished and the work needed to be done. The number of patients started to drop in the villages, although we easily would see 100 a day; though this sounds like a lot, the critical nature of the problems changed. Occasionally people were still being carried out of the mountains by friends with injuries they sustained during the earthquake. Simple cuts turned into cellulitis and the osteomylitis. An example was an old man who came to me clinging onto a friend's back, he could not walk and one glance at his left foot showed me why. The foot, damaged in the quake, was five times larger than the right; it also had two infected wounds that smelled terrible. He asked me not to cut off his foot. I told him we would do everything to save his life first, then save his foot. We dealt with pain and hemorrhaging during childbirth, colds and flu, constipation, diarrhea, fever in infants, adolescents and adults, plus one man who said his urine was yellow; when I told him to drink more water, he replied that "the water was too cold" and walked out of the tent.
I have been privileged to teach the NADA protocol to Pakistani Army personnel, medical students from the U.S., two psychologists and a few Pakistani nationals. It is funny to see a man doing auricular acupuncture with a machine gun strapped to his back, but I saw it often and the results were good. This was a beginning. I reminded all I worked with that psychological issues take time to heal, and the NADA protocol - with counseling, family and community support - was a great way to help start the healing process. I was able to leave everyone I worked with a few cartons of needles, and I have more to bring back with me upon my return.
The job in Pakistan is far from over. I have spoken with acupuncturists in California who want to go to Kashmir to assist in this cause. We are looking for people who not only have a LAc or DOM degree, but people who, like myself, have a Western medical background, be it an EMT, paramedic, nurse, etc. There is a need for people who believe in a holistic approach to medicine, especially during the acute and subacute phases of this project. Combining Eastern medicine to help Western medicine work better is a beneficial and exciting approach to patient care; one that not only benefits the body, but also the soul. This has been a very positive way to expose Eastern medical science to physicians who have never been exposed to Oriental medicine as they rotate through the camp. I have had the chance to show many doubting physicians, health care workers and reporters that acupuncture can make a difference in the outcome of many problems. The best part was that when they saw it work, they would then ask if I would train them in the NADA protocol.
I believe there is a window of opportunity in every disaster - an opportunity for change even in old, fixed systems. Action needs to be taken right away and followed up on. We, as acupuncturists, can teach others how cooperation and mutual respect for each others' skills benefits not just one group, but our medical community as a whole.
There is another reason for wanting people to have a hand in both camps. The day we left for Islamabad, we learned that a bus went over the side of a high road. The army asked for and transported our medical team to the scene of this terrible accident. Twenty-two people were killed; others were severely injured. You'd think that with all the trauma these people had gone through, they should get some kind of break. The news sent my heart plummeting into its own abyss.
Phases two and three are now running into each other and will continue to do so for a short time. As teams go into the field and treat patients, those in the base camp continue making improvements on the field hospital clinic, ER and pediatric units. The army is opening more roads and allowing more villages to be accessed. There is a wonderful commitment by the founders of Operation Heartbeat to see this project through, and I am happy to have been a part of it. My commitment to service in relief efforts runs deep. I hope that people who want to work for the betterment of others, and those who are willing to challenge themselves, will contact me and leave me their contact information so I can begin a database of LAcs who would go to the front lines of disaster relief work.